Characteristics and Clinical Ocular Manifestations in Patients with Acute Corneal Graft Rejection after Receiving the COVID-19 V...
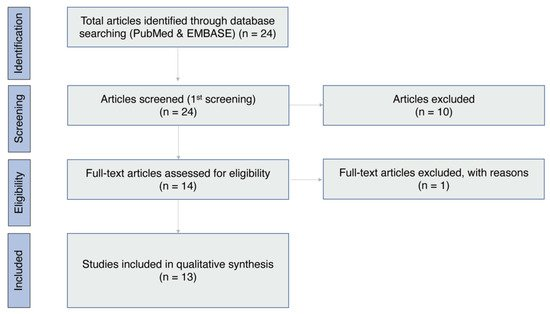
This study aimed to determine the characteristics and clinical ocular manifestations of acute corneal graft rejection after coronavirus disease 2019 (COVID-19) vaccination. We conducted an online search of the PubMed and EMBASE databases. Data on recipient...

You bring up a good point. I think the answer to your questions can be inferred from the data.
The study is focused on corneal transplant rejection following covid inoculation of the transplant recipient. Average time of rejection was within 3 weeks post jab. Average transplant age was about 2 years with a couple of them being at least 20 years. So, I think that would be a good indicator that the bulk of these transplant rejections are from unjabbed donors since the age of the transplants would put the donor outside of the vaxxine rollout timeframe. Therefore, tissue rejection is directly correlated to receiving the jab. If the rejection were related to receiving contaminated donor tissue, the rejection would have occurred immediately post transplant.
It also appears that increased risk factors for corneal transplant rejection are multiple transplants, possibly two eyes, along with complications. In addition, comitant autoimmune disease may increase risk of rejection following mRNA jabs.
I have an aunt with bilateral corneal transplants. I am passing this information along to her to give her something to consider if she is thinking of getting boosted. She already has had a massive RA flareup following the initial jabs. There were also complications following her second transplant - something I am sure she does not want to repeat.
“the dampened inflammatory responses to the vaccine may have reduced the immune stress on these grafted organs. Therefore, prescribing oral immunomodulators or increasing the frequency of topical steroid administration should be considered for allograft recipients with a high rejection risk”
Most organ transplant recipients are prescribe immune-modulatory medications for life in order to ensure the body doesn’t reject the organ. She may want to ask her doctor next time she goes in!
Corneal transplant patients are given anti-rejection eye drops that usually contain ciclosporin. Any transplanted tissue will be rejected without immunosuppressants.
The way I read the study was to either need to increase the frequency or keep them on longer? The drops aren’t forever like a heart transplant?
I am not an expert in this area. But the types of meds given and their duration depend on the case. My aunt, because she had complications after her second surgery, has to continue with the immunosuppressant eye drops. It certainly is different than a heart transplant that requires antirejection meds for life. Immunosuppressants are a double edged sword. They often deal with one issue to in turn create other issues. Damned if you do, and damned if you don't.